
 Descargar número completo
Descargar número completo Download full issue
Download full issueCITA ESTE TRABAJO
Alonso Belmonte C, Parra López B. Large intrathoracic collection secondary to acute chronic pancreatitis displacing large hiatal hernia, an uncommon presentation. RAPD 2024;47(2):84-86. DOI: 10.37352/2024472.5
Introduction
Chronic pancreatitis arises as a consequence of repeated acute inflammatory insults to the pancreas, resulting in endocrine and exocrine dysfunction requiring replacement treatment. It is associated with a wide range of symptoms1 , including diarrhoea due to maldigestion of protein-rich food because of a deficiency of the enzymes necessary for its metabolism.
However, episodes of acute chronic pancreatitis may occur, with decompensation of the already impaired baseline pancreatic function2. Clinically, such episodes manifest with abdominal girdle pain in the epigastrium, together with mild elevation of acute phase reactants and hyperlipaemia with less marked elevations than in acute pancreatitis.
Imaging usually shows an atrophic pancreas with minimal oedema and rarefaction of adjacent fat, with the possibility of peripancreatic collections and collections at the level of the splenocolonic ligament. An uncommon location of these collections is at the intrathoracic level3 , which compresses the usual anatomical structures at that level, generating a space compromise that the patient may manifest clinically with dyspnoea.
Due to the infrequency in clinical practice and in the literature of this intrathoracic presentation, we present the clinical case of a 60-year-old woman with chronic alcoholism and chronic liver disease, who is diagnosed with chronic pancreatitis complicated by an intrathoracic collection that displaces the known hiatal hernia and other structures, with significant clinical repercussions.
Clinical Case
A 60-year-old patient with a history of chronic alcoholism and chronic liver disease, who attended the emergency department for abdominal girdle pain in the epigastrium, radiating for 3 days, with no other associated symptoms. She mentioned that she had presented the same symptoms on other occasions, having been diagnosed with acute pancreatitis on previous admissions based on clinical and analytical criteria.
Analytically, there was an increase in acute phase reactants (CRP 50 mg/dL Leukocytes 13500 mm3 at the expense of neutrophilia (8500mm3)) as well as hyperlipidaemia (1300 mg/dL), ruling out intercurrent infectious symptoms due to organs and systems.
The patient, presenting clinical and analytical criteria for a new episode of acute pancreatitis, was admitted to the Digestive Department for evolution and monitoring.
Figura 1
Coronal CT scan of the abdomen showing an intrathoracic collection associated with gastric chamber herniation, which is displaced superiorly and medially by the collections.

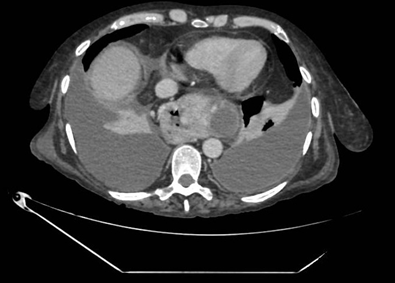
Figura 2
Cross-sectional abdominal CT scan showing gastric herniation together with collections secondary to acute chronic pancreatitis. In addition, bilateral pleural effusion and collapse of the lower lung lobes due to space conflict are seen.
During hospitalisation, the patient began to present dyspnoea on medium exertion that evolved to minimal exertion in a few days, together with persistent abdominal pain and oral intolerance, and it was decided to perform a thoracoabdominal CT scan to rule out complications.
A thoracoabdominal axial tomography was performed, which showed portal hypertension and splenomegaly due to known chronic liver disease, as well as findings that raised suspicion of chronic pancreatitis (presence of atrophic pancreas), in turn complicated by thrombosis of the splenic vein and multiple well-defined and encapsulated collections. These collections are distributed along the tail of the pancreas, the spleno-colonic ligament and at the retrogastric level. The herniation of the latter together with the gastric chamber towards the thorax is striking, causing a displacement of the latter superiorly and medially, data that would justify the patient's symptoms. Free intraperitoneal fluid, bilateral pleural effusion and collapse of the lower lobes were also observed.
Following tomographic findings, medical treatment was intensified, an absolute diet was maintained and parenteral nutrition was started in order to meet caloric and protein requirements, with close monitoring of the collections described. The clinical evolution was satisfactory, with clinical improvement, decrease in reactants and stabilisation of the collections, some of which decreased in size, especially the intrathoracic one.
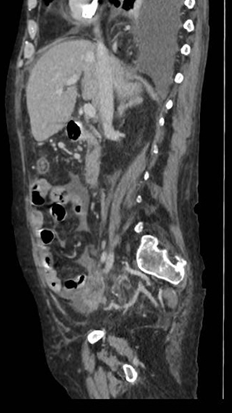
Figura 3
Sagittal CT scan of the abdomen showing an intrathoracic collection. Other collections are also seen at the retrogastric level, in the tail of the pancreas and in the splenocolonic ligament with no signs of complication.
Finally, on consolidation of the clinical, analytical and radiological improvement, the patient was discharged without requiring any invasive therapeutic measure, with outpatient follow-up of the collections described. Enzyme replacement therapy was added to the usual chronic treatment for findings of chronic pancreatitis, with dosage adjustment in consultations.
Discussion
Chronic pancreatitis is an entity that should be suspected in patients presenting with repeated episodes of acute pancreatitis susceptible to hospital admission. This pathology presents clinical (abdominal pain, exocrine/endocrine insufficiency, nutritional deficits, among others), analytical (elevated acute phase reactants and hyperlipaemia, but to a lesser extent than in isolated cases of acute pancreatitis) and radiological criteria that support its diagnosis.
In this case, an atypical clinical presentation of acute chronic pancreatitis, namely intrathoracic collections, has been reported. After an exhaustive review of the literature, cases of acute pancreatitis secondary to herniation of the pancreas at the thoracic level have been found, although the literature is scarce with respect to the presence of collections at this level.
For this reason, in the case of a patient with abdominal pain typical of pancreatitis associated with dyspnoea and persistent oral intolerance, it is essential to rule out complications intrinsic to the underlying pathology, such as intrathoracic collections, as part of the broad differential diagnosis that must be established. The complication observed in this case, given the infrequency of its manifestation, represents a diagnostic challenge that must be taken into account in daily clinical practice.