
 Descargar número completo
Descargar número completo Download full issue
Download full issueCITE THIS WORK
García Robles A, García Ortiz JM. Update on the management of pT1 colorectal cancer. RAPD 2024;47(3):102-115. DOI: 10.37352/2024473.2
Current management of pT1 CRC. Histological risk criteria.
Colorectal carcinoma (CRC) pT1 is the earliest form of CRC. It is defined as a tumour where neoplastic cells growing within a polyp invade the submucosa through the muscularis mucosae, but do not overgrow it. Endoscopic resection of a pT1 CRC is only oncologically safe if it is assumed that the malignant cells have not metastasised to locoregional nodes. Otherwise, surgical resection is considered necessary with the intention of preventing distant metastasis. Since in a local resection the lymph nodes are not removed and therefore cannot be analysed, a prediction of the risk of lymphatic metastasis (LM) is necessary and is based on the anatomical pathology report, where the presence or absence of the following histological criteria should be described:
Degree of differentiation: this refers to the resemblance of the tumour cells to normal colonic epithelium and is defined according to the glandular structure content of the tumour[10]. Tumours with more than 50% of glands are well or moderately differentiated (GI and G2), considered low grade and with a favourable prognosis. Those with less than 50% glandular formations are poorly differentiated (G3), this being an independent risk factor for poor prognosis[11],[12].
Lymphovascular invasion: the presence of tumour cells within the blood vessels of the submucosa, and especially the lymphatic vessels, is a known risk factor and is in fact the histological criterion that most strongly correlates with the presence of lymph node metastasis [12]-[14].
Tumour budding (BT): indicates the presence of a tumour cell or groups of up to four tumour cells aggregated at the invasive tumour front. There can be three grades of BT: low, intermediate and high. High grade BT has been shown to be a histological risk factor for ML in pT1 CRC[15],[16], although it is only described in less than half of the published studies [9].
Resection margins: most Western guidelines recommend a margin of safety >1 mm to consider a curative resection (R0)[17],[18], based primarily on the results of one study that observed residual invasive disease in 16% when the polypectomy margin was <1 mm, in 21% with an indeterminate margin (Rx resection) and in 0% when the margin was ≥1 mm (p=0.009), but this was not a risk factor for ML[19].
Depth of submucosal invasion: the degree of submucosal invasion is categorised differently depending on the morphology of the polyp, according to the Haggitt and Kikuchi classifications (Figure 1):
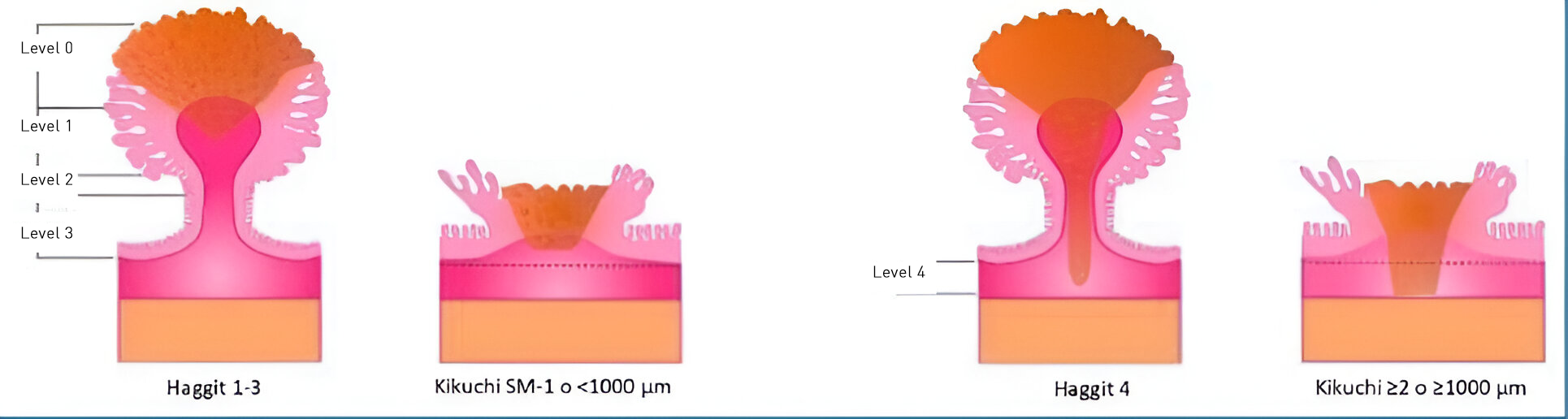
- Haggitt classification[20], used for pedunculated polyps, classified into four levels according to the level of submucosal invasion: Haggitt 1: submucosal invasion at the head of the polyp; Haggitt 2: invasion up to the junction of the head with the stalk; Haggitt 3: invasion up to the stalk of the polyp; and Haggitt 4: invasion into the deep submucosa, below the stalk into the underlying colonic wall, which is considered a risk factor for lymphatic metastasis.
- Kikuchi classification[21], for non-pedunculated lesions: the submucosa is divided into three levels according to the degree of submucosal infiltration: SM-1 (<1,000 microns), SM-2 and SM-3 (>1,000 microns). The Kikuchi level can only be reported when muscularis propria is included in the resection specimen, which is not the case in many cases.
A polyp has superficial submucosal invasion if the invasion is <1,000 μm (Kikuchi SM-1) or, in case of pedunculated polyps, Haggitt level 1-2-3. Deep submucosal invasion of >1,000 μm (Haggitt 4 or SM 2-3) has been associated with a higher risk of lymph node invasion, and therefore worse prognosis. This relationship is based on results from historical surgical series[22].
Surgery or follow-up? The great dilemma
The final decision on whether a patient should be referred for further surgery after local resection of a pT1 CRC or follow-up depends mainly on the histological criteria described above. As recommended in clinical practice guidelines[23]-[26], a pT1 CRC is considered high-risk, and therefore an indication for salvage surgery, when one or more of the histological risk criteria are present. The surgical technique varies depending on the location of the tumour, but always includes resection of the corresponding meso, with the vascular pedicle and the lymphatic drainage system that includes the locoregional lymph nodes of the resected segment.
The scientific evidence supporting this recommendation to date is based on the results of previous studies showing that, in the absence of these histological criteria, the risk of residual local neoplasia is 0.7%, the risk of lymphatic metastasis is less than 1%, and the risk of distant metastasis is around 0.7%. In contrast, in the presence of any of these, the risk was 4-11%, 10-16% and 1.3-6%, respectively[24],[27]. These estimates do not take into account the different relative risk that histological criteria show in the series, nor the possible effect of combining these criteria with each other.
"Sub-optimal" histological criteria:
Using current histological criteria, more than 80% of patients with pT1 CRC are classified as high risk[31]. However, after histological analysis of surgical resection specimens, only 2-10.5% have lymph node invasion and less than 20% have residual lesion[29],[32]-[37]. Therefore, there seems to be a risk of overtreatment by relying exclusively on histological criteria for our decision making, as we are referring many pT1 CRC to surgical rescue that could have been optimally treated endoscopically. On the other hand, there are a number of limitations that may hinder decision-making, such as the lack of information in the anatomopathological description or inter-observer variability. Thus, in the work of Lugli et al.[38], 67 histological reports after local resection of pT1 CRC were reviewed, showing that histological grade was only reported in 31% of cases, tumour budding was not reported in 97% and lymphovascular invasion was not described in 81%. On the other hand, regarding inter-observer variability, Rampioni et al.[39] retrospectively analysed 82 endoscopically resected pT1 CRCs: in 9.7% of the cases there was a change in the classification of the risk of lymphatic spread of the lesions after review by a second pathologist, 7.3% were reclassified as high risk and 2.4% as low risk after a 2nd assessment.
There is a general consensus in clinical practice guidelines to consider the presence of lymphovascular invasion, the degree of histological differentiation and tumour budding as independent risk factors for lymphatic spread. However, recent evidence questions the other criteria: deep submucosal invasion and resection margin:
- Deep submucosal invasion: in a retrospective population-based cohort study[12] that prospectively collected data from 1,439 patients with T1 CRC resected locally by surgery from two populations (Sweden, between the years 2009-2017 and Denmark, between 2016-2018) it was observed, in contrast to that reported in previous studies, that differences in the risk of LM in patients with superficial submucosal invasion (SM-1) versus deep submucosal invasion (SM-3) were very limited, concluding that deep submucosal invasion is not an independent risk factor for lymphatic invasion. In 2022, the Dutch group led by Evelyn Decker, published a meta-analysis[40] that included 67 studies with 21238 patients where it was also shown that deep submucosal invasion, when appearing as the only risk factor, has an absolute risk of LM of only 2.6%, and in multivariable analysis was not a significant predictor of LM (odds ratio [OR] 1. 73; 95% confidence interval [CI] 0.96-3.12), compared to the presence of the other factors that did show significant association: poorly differentiated histology (OR 2.14; 95% CI 1.39-3.28), lymphovascular invasion (OR 3.16, 95% CI 1.88-5.33), high-grade tumour budding (OR 2.83, 95% CI 2.06-3.88).
The question we should be asking is whether a 2.6% absolute risk of lymphatic metastasis is sufficient to refer a patient for surgery. We should bear in mind that oncological surgery does not prevent mortality and recurrence 100%: In the retrospective study by Tamaru et al.[41], a recurrence rate of 3.8% was observed, and CRC-associated mortality was 1.2% in cases of pT1 CRC treated with primary surgery alone. Surgical treatment for non-malignant colorectal polyps has been associated with 1% mortality and high morbidity rates, especially in the elderly population, in whom endoscopic treatment could ensure a better quality of life compared to surgery [42].
- Deep resection margin <1 mm: The most accepted definition of an affected resection margin or incomplete resection (R1) is one in which the distance to diathermy-induced histological change is less than 1 mm[43], based on results from several studies[44]-[47] showing an increase in residual disease (7-17%). But recent evidence is beginning to question this: A retrospective study from the Dutch pT1 CRC group[48] showed that a free resection margin <1 mm (between 0.1 and 1 mm), in the absence of other risk factors (high-grade budding, lymphovascular invasion and poorly differentiated histology) has a risk of residual neoplasia of only 2.9% (95% CI 1.0-6.7), with no significant difference compared to lesions with margins >1 mm. Furthermore, analysing lesions with resection margins <1 mm and with residual disease, the presence of tumour budding was also demonstrated in 80% of them.
The European Society of Gastrointestinal Endoscopy (ESGE) clinical practice guideline on endoscopic submucosal dissection states that there is no evidence to support the concept that a tumour-free margin of less than 1 mm should be considered positive and, therefore, an indication for surgery, recommending the concept of "preferably >1 mm" to define R0 resection, taking into account that if it is < 1 mm but free of tumour and without other risk factors, close follow-up could be considered[49].
On the other hand, it seems that the risk of residual disease is more related to incomplete resection than to the status of the margins. Thus, studies that had reported high rates of residual disease (>15%) after endoscopic resection of pT1 CRC had included incomplete endoscopic resection techniques in >10% of them. In contrast, studies with low rates of residual disease mostly excluded incomplete resections[43]. In addition, fragmented endoscopic resection, which is often performed to resect polyps >20 mm in size, is often reported as an indeterminate resection margin (Rx resection) even though it is a complete resection, which may result in a referral for surgery as it is erroneously considered an incomplete resection [43].
Does surgery really improve the prognosis of pT1 CRC?
pT1 CRC generally has an excellent prognosis, with 5-year overall survival rates of 94%[35], so surgery may have a potential beneficial effect only in a small group of patients. We therefore wonder what is the best therapeutic strategy in patients with pT1 CRC, whether the treatment modality (endoscopic or surgical) influences prognosis. In the meta-analysis by Dang et al.[30], recurrence and mortality related to pT1 CRC were analysed: 71 studies with 5,167 patients with pT1 CRC treated with endoscopy alone were included and an overall recurrence risk after endoscopic resection of 3.3% after 72 months of follow-up, with the cumulative incidence of recurrence in patients with low-risk pT1 CRC being 0.7% (0.4-1.2%) and 7% (4.9-9.9%) for patients with high-risk pT1 CRC. These figures are similar to those reported for patients with surgically treated pT1 CRC: in the meta-analysis by Yeh et al[35] there was no significant difference in overall survival rates, recurrence-free survival or CRC-specific survival between patients with high-risk pT1 CRC treated with endoscopy versus those treated with surgery alone. Therefore, it appears that neither endoscopic treatment nor surgery will change the unfavourable prognosis in high-risk pT1 CRC. One possible reason for this is that the likelihood of an unfavourable prognosis may be more related to the aggressiveness of the tumour itself than to the treatment performed[43]. Prospective long-term studies are needed to provide more data and to help us make decisions about follow-up in patients with high-risk pT1 CRC treated endoscopically.
Another important aspect to consider in our decision-making is the risk of adverse events (AE) of the treatment offered to patients with pT1 CRC. It is estimated, based on data from European screening programmes, that the percentage of pT1 CRC treated with surgery is currently between 38-55%[36],[50],[51]. An otherwise healthy patient who has had a potentially curable malignant polyp resected endoscopically will be highly likely to be referred for surgery, with the risk of AE that this entails, as well as the added costs.
Table 1 summarises the main AE's of endoscopic treatment, with an overall percentage of 5.5%, which is much lower than the 20% morbidity related to surgical treatment, and which is similar to that observed in more advanced stage CRC surgery[35],[51],[52]-[54].
Table 1
Morbidity and mortality of endoscopic treatment vs surgical treatment of pT1 CRC.
| Adverse events | Mortality | |
| Endoscopic treatment |
5.5% Bleeding 3.78% Perforation: 1.2% Postpolypectomy 0.6% | 0-1.4% |
| Surgery |
20% Severe AEs 8% Anastomotic leak 4% | 3.2% |
The meta-analysis by Yeh et al.. also reported a much lower AE rate among patients treated with endoscopic resection (2.3%) compared to those treated with primary surgery (10.9%), with the differences being statistically significant (p<0.001)[35]. With respect to mortality, differences are also evident: in the study by Belderbos et al.[51], mortality in patients treated with surgery was 3.2%, which contrasts with 1.4% in the group treated with endoscopy, taking into account that in many studies mortality in these is around 0%[32],[53],[54].
Endoscopic evaluation
Endoscopic evaluation of any colorectal lesion is considered a fundamental element in deciding the most appropriate resection technique[55]. Optical diagnosis allows us to estimate the probability of submucosal invasion of a colorectal lesion, as well as the depth of this invasion. If pT1 CRC is suspected during colonoscopy, en bloc resection should be performed, which will then allow adequate histological evaluation and optimal staging. In the endoscopic evaluation of a colorectal polyp, we must take into consideration the following characteristics that may suggest the suspicion of occult carcinoma:
Size: the risk of invasive cancer increases progressively the larger the size of the lesion. According to a meta-analysis of more than 5000 adenomas, this risk is 9.2% for lesions between 20 and 30 mm, and increases to 16.5% for lesions larger than 30 mm in diameter[56].
Location: Several studies have shown that location in the left colon, and especially in the sigma and rectum, is an independent risk factor for developing pT1[57],[58].
Morphology:The Paris[59] and Kudo classifications of lateral spreading tumours (LST)[60] are very useful for estimating the risk of malignancy of a lesion: homogeneous granular LSTs have a very low risk of only 0.5%. LSTs with mixed granular surface (with dominant nodule or non-granular areas) the risk of malignancy increases to 10.5%[56] (Figure 2).
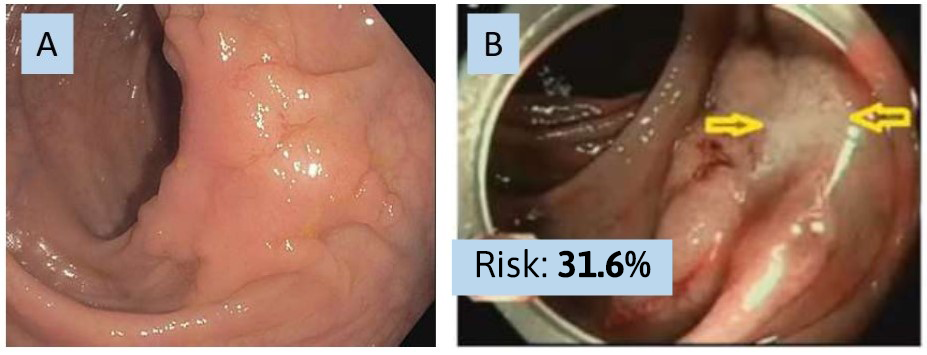
Non-granular LSTs (nongranular LST-NG) have a higher risk of deep submucosal invasion and, if they have a pseudodepressed area, the risk increases to 31.6%; 95% CI 19.8 %-43.4 %[56], (Figure 3).
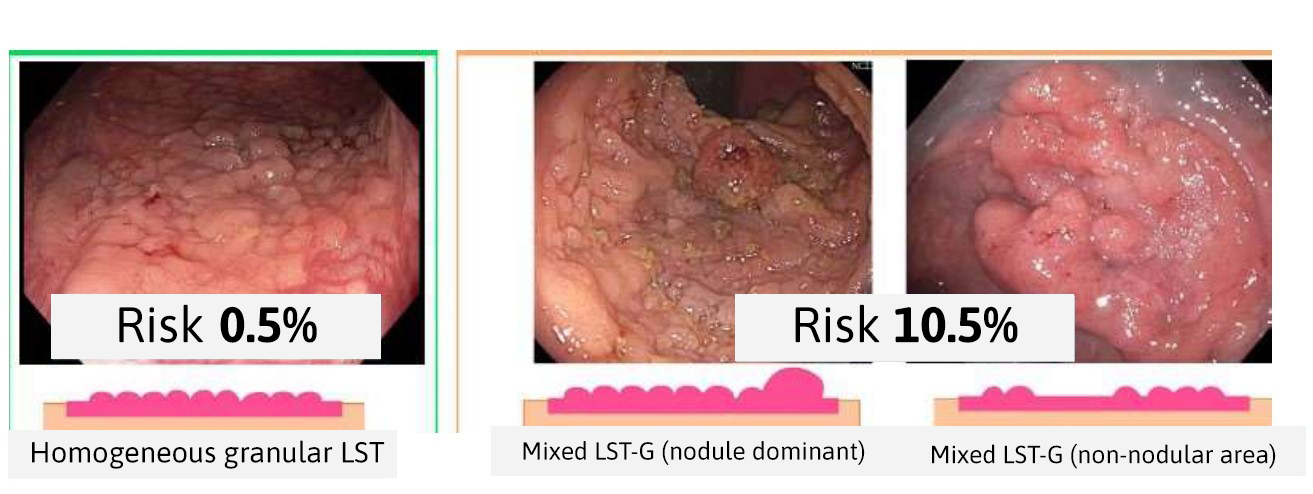
Figure 3
Las lesiones de extensión lateral no granulares (LST-NG). A): LST -NG plano elevada (0-IIa). B) LST-NG con área pseudodeprimida: el riesgo de invasión en profundidad se incrementa hasta el 31.6%[56].
Macroscopic features: as a colorectal polyp becomes more dysplastic, angiogenesis increases and changes occur in the microvasculature that we can identify and thus estimate a possible deep submucosal invasion: presence of surface erythema or spontaneous bleeding[61], erosions, ulcerations or exudate on the surface of the polyp[62],[63]. Other signs of malignancy may include retraction/convergence of folds, the presence of so-called "chicken skin" and the "no-lifting sign", which can be observed when the lesion does not rise after submucosal injection, although these alone lack specificity[64],[65].
Glandular and vascular pattern: unlike the other features, which can be assessed by white light endoscopy, assessment of the distribution pattern of glandular crypts and vessels on the surface of the lesion requires the use of virtual chromoendoscopy. The NICE classification allows differentiation of serrated or hyperplastic lesions, adenomatous lesions and/or cancer with advanced invasion[66],[67], allowing the endoscopist to decide whether a lesion is a candidate for endoscopic treatment or requires surgical oncological resection, with good confidence in up to 87.5% of lesions[68]; But for the rest, other advanced imaging techniques would be needed, such as optical magnification, with which we can apply other classifications: JNET, Kudo or Sano: The presence of an irregular vascular and crypt pattern (JNET 2B, Kudo Vi, Sano IIIA) suggests superficial submucosal invasion, which could be treated by endoscopic (en bloc) resection. When this pattern is completely lost (JNET 3, Kudo Vn, Sano IIIB), it is most likely an infiltrative lesion[69]-[71] (Table 2).
Table 2
Advanced imaging classification systems and the different subtypes/categories associated with the presence of pT1 CRC with deep or superficial invasion.
Despite advances in optical diagnosis, evidence shows that in actual practice around 42% of endoscopically resected pT1 CRC are unexpected histological diagnoses[72]. In scans performed by expert endoscopists, this rate drops to around 10-15%[65], and in some studies performed in non-expert endoscopists, the percentage of unidentified T1 CRC can be as high as 80%. Inadequate assessment of the risk of invasion of a lesion may have negative repercussions for the patient, such as fragmented resection of a malignant lesion and subsequent inability for adequate histological examination, which may lead to surgery and loss of the opportunity for local, organ-sparing, curative resection[73]. Another consequence of a failed endoscopic assessment may be the need for repeat colonoscopy to tattoo the resection site of a malignant lesion or the erroneous indication of surgery for benign lesions.
The case of pT1 in the rectum
Lesions located in the rectum present a higher risk of occult submucosal invasion than in the rest of the colon. This risk is especially significant in the case of non-granular or mixed surface LSTs with a sessile component[58]. For large mixed granular LSTs larger than 4 cm, the risk of occult submucosal invasion is three times higher in the rectum than in the rest of the colon[57]. Furthermore, rectal location appears to confer a higher risk of lymphatic metastasis, and is a risk factor for recurrence after local resection, the more distal the lesion is located, the higher the risk [74],[75].
On the other hand, rectal surgery has a greater impact on patients, given the greater likelihood of complications and sequelae that negatively affect the patient's quality of life, such as the possibility of faecal or urinary incontinence, temporary or permanent stoma, or sexual dysfunction[76].
In summary, the consequences of unnecessary surgery in the particular case of the rectum may be worse, which, together with a greater risk of hidden deep submucosal invasion and its greater anatomical accessibility, would tip the balance in favour of local en bloc resection techniques in lesions where the risk of invasion is not negligible.
Local resection techniques
There are several local and minimally invasive methods that allow curative treatment of pT1 CRC. The choice of the most appropriate one may vary according to its capacity to resect the lesion en bloc, as well as its complication rate, its cost and duration, and its availability, among others.
- Endoscopic Mucosal Resection (EMR) or Mucosectomy: allows resection of low-risk lesions in fragments, such as homogeneous granular LSTs located in the right colon. However, for lesions with risk of deep invasion and that, therefore, would require en bloc resection, this technique is only effective in lesions < 20 mm in diameter. There are other derivative techniques, such as underwater EMR or partial or total mucosal precutting, which in expert hands, increase en bloc resection rates in lesions up to 25-30 mm. Its better safety profile, as well as its lower time and resource consumption, makes EMR available in almost all centers[77].
-Endoscopic Submucosal Dissection (ESD): unlike EMR, it allows en bloc resection (R0) regardless of the size and location of the lesion, obtaining a high quality histological specimen and considerably reducing recurrences and the need for revision and retreatment endoscopies[49]. In lesions with superficial submucosal invasion, ESD achieves en bloc resection rates of over 90%. When performed in lesions with deep submucosal invasion the R0 resection rate drops to 47-64%[78],[79]. It is necessary to take into account the complication rates with the need for additional surgery, such as perforation (around 5%) or delayed hemorrhage, which occurs in up to 20% of cases[80]-[85]. Furthermore, theoretical and technical training in ESD requires a high degree of specialization and its learning curve is slower than that of other techniques, which, together with the fact that it is a procedure of prolonged duration, means that in Western countries its availability is heterogeneous[86].
-Intermuscular dissection: variant of ESD where the dissection plane is not located in the submucosa, but in the connective tissue that separates the longitudinal and circular layer from the muscular layer, including the external, circular layer in the specimen. It has only been shown to be technically possible in the rectum, where it could exceed 80% en bloc resection of lesions with deep submucosal invasion [87].
-Transmural endoscopic resection (full-thickness resection: FTR): allows obtaining an optimal histological specimen by including the complete muscular layer, which in turn allows resection en bloc of lesions with deep submucosal invasion. It is a fast technique, assisted by a device with a cap that is attached to the tip of the endoscope, which with a short learning curve allows R0 resections in approximately 90% of lesions up to 15 mm in diameter[72]. Above 20 mm the ability of this technique to resect en bloc drops drastically. The AE rate is 8-14%, including 2-3% of deferred perforations due to premature opening of the ovesical clip[73]. With the new evidence available, the involvement of the resection margins tends to be considered more a risk factor for local recurrence than a criterion for high risk of LM, which favors the possibility of using this technique to perform an additional resection on the eschar of a previously resected invasive lesion with affected margins or margins that cannot be assessed by fragmentation. This has been the most frequent indication for transmural resection in the Dutch T1 CRC cohort, where 77.6% of eschar resected by this technique showed no residual tissue. Further analysis suggests that when this is the case, the probability of LM and/or recurrence is similar to that of those patients who undergo surgery[74], and may therefore be considered an alternative to surgery in the absence of other risk factors.
-Transanal Minimally Invasive Surgery (TAMIS), with the aid of a single port placed in the anus, laparoscopic instruments can be used to resect lesions located in the middle and proximal rectum, including the muscular layer, and can therefore be useful in cases of suspected deep invasion or for the resection of eschar. TEM (Tranasnal Endoscopic Microsurgery) is another local resection technique comparable to TAMIS, although it uses different surgical instruments. The en bloc resection and complication rates of TAMIS/TEM may be similar to those of ESD. There is currently an ongoing randomized clinical trial (TRIASSIC) to compare both techniques in the rectum [91].
In summary, when a lesion is suspicious or presents a significant risk of being a pT1 CRC, we have several minimally invasive local resection techniques with the main objective of organ preservation, especially in the rectum, and also with an acceptable safety profile, which allow en bloc resection of the tumor and an adequate assessment of the histologic risk of LM. The patient's characteristics and preferences, as well as the size and location of the tumor and local availability and experience will determine the most appropriate strategy in each case.
Decision-making after local resection of pT1 CRC
The main objective in the follow-up of endoscopically resected pT1 CRC is to identify local recurrence or metachronous lesions at a time when additional treatment could extend the patient's survival or improve his quality of life. When faced with a patient who has had a pT1 CRC resected, in order to make the decision to follow up or, on the contrary, to refer the patient for surgical rescue, three factors must be taken into consideration:
1. Risk of LM, established by histologic criteria. The limitations of the considered suboptimal criteria (deep submucosal invasion and resection margin < 1mm) should be taken into account as independent risk factors for LM, according to current evidence.
2. Comorbidities, patient's physical condition and risk of adverse events.
3. Patient preferences and impact on quality of life.
It is essential that decision making be discussed within a multidisciplinary committee, where these factors, especially the individual perioperative risk of each patient, will be taken into account to help us decide who will really benefit from additional surgical treatment. Scales developed to assess the risk of AE according to a patient's comorbidities and life expectancy are very useful. The most widely used is the Charlson Comorbidity Index (CCI)[92]. Age older than 79 years and a CCI >3 points are associated with shorter survival[93]. On the other hand, according to the Modified Frailty Index (FI), frail patients with a FI ≥2 points present increased morbidity-mortality rates, fewer discharges, more readmissions and lower disease-free survival and overall survival rates[94].
In the following sections we will summarize the main recommendations for follow-up after endoscopic resection of pT1 CRC that have been developed by the main scientific societies of digestive endoscopy in Europe (ESGE)[26],[49] and the American Gastroenterological Association (AGA)[95] to help us define under what circumstances additional treatment would improve patient survival. Its low level of evidence must be taken into account, so we also add the recommendations of the latest studies and meta-analyses with the most recent evidence.
Low risk pT1 CRC: it is considered curative resection and does not require additional procedure or treatment.
- There is no evidence to support the periodic determination of carcinoembryonic antigen (CEA) or imaging tests, neither for initial staging nor during follow-up. The National Comprehensive Cancer Network (NCCN) guidelines specify, in relation to stage I CRC, that "imaging is not routinely indicated, and should only be based on symptoms and/or clinical concern for recurrent/metastatic disease" [96].
- Endoscopic follow-up is indicated (always based on a quality baseline colonoscopy, complete up to the cecum and with adequate cleaning):
The ESGE recommends[26]: 1st colonoscopy at one year, then at three years and at five years after the previous one. In the case of a non-pedunculated lesion resected in fragments, the first endoscopic revision should be performed between 4-6 months. The AGA recommends[95]: 1st colonoscopy in 3-6 months. 2nd colonoscopy: six months after the previous one. 3rd colonoscopy: one year after the previous one. Continue thereafter according to post-polypectomy recommendations.
High risk pT1 CRC:
In a recent meta-analysis by Dang et al[30] that included 71 studies with more than 5,000 endoscopically treated pT1 CRC, an overall recurrence risk of 3.3% was established, with most cases of recurrence (95.6%) occurring in the first 72 months. When categorizing pT1 into two groups, high and low risk, a recurrence of 7.7% was observed in the high risk group and only 0.7% in the low risk group. These findings suggest that histologic status is the most important factor in establishing follow-up recommendations.
However, in contrast to low-risk pT1 CRC in which clinical practice guidelines do give more specific follow-up recommendations, in the case of high-risk pT1 CRC it is more difficult to establish more specific follow-up guidelines, mainly due to the heterogeneity of this group of patients. Moreover, not all histologic criteria have the same weight in determining risk stratification, as is the case with the so-called "non-consensus" criteria that we have discussed in this article: deep submucosal invasion12,40 or distance to the deep margin of <1 mm[48].
In view of the lack of quality prospective studies with long-term follow-up periods in patients with high-risk pT1 endoscopically resected, we will continue to base our decisions on histological criteria, but it is also important to pay attention to other relevant clinical characteristics that would increase the risk of recurrence[35]: rectal location, non-pedunculated lesion morphology, fragmented resection not en bloc ( EMR more risky than ESD).
We can conclude that in the case of patients who have undergone resection of a high-risk pT1 CRC, we should try to carry out the most personalized follow-up possible, with colonoscopies, imaging tests and periodic CEA determination, with the aim of detecting local and distant recurrence, at least during the first six years, the period in which most cases of recurrence have been shown to occur[30]. There is no consensus in the guidelines on the periodicity with which the different tests should be requested. It has not been demonstrated that "intensive" follow-up improves survival[97]-[99] and, in addition, there is the probability of incidental findings in imaging tests that in many cases may be clinically irrelevant and cause more anxiety in patients, as well as increased costs. A recently published study[100] showed a 5-year cumulative incidence of benign incidental findings of 18.3%, which contrasts with a 2.5% 5-year cumulative incidence of malignant incidental findings during follow-up.
pT1 resected in the rectum:
The risk of recurrence after local resection is higher for rectal pT1s, standing at 7.7%[101], much higher than the 3.3% for pT1s of any other colon location treated endoscopically[30]. Stratifying according to histologic status, the risk of recurrence of high-risk rectal pT1 is significantly increased after local resection: 12.5% (if resected endoscopically) and 29.7% (if resection is via TEM/TAMIS). With these results we could think that the best solution is surgical rescue. But we must also take into account the negative impact that oncologic surgery on the rectum can have: risk of incontinence/sexual dysfunction, consequences of a possible low anterior resection syndrome or abdomino-perineal amputation.
pT1 in low-risk rectum: close follow-up should be offered, preferable to surgery, since a priori the negative consequences of oncological surgery would outweigh the possible benefits. The Dekkers meta-analysis[101] proposes a 5-year follow-up strategy: Rectoscopies every 6 months for the first two years, then annually for the following five years, with annual CEA determination.
pT1 in high-risk rectum: the patient should be offered complete surgery with total excision of the mesorectum, as indicated in most clinical practice guidelines[49],[95],[102]. If oncologic surgery is not possible (the patient refuses surgery or is at high surgical risk), intensive follow-up should be performed for at least 5-6 years in order to detect endoluminal recurrence, locoregional lymphatic metastases and/or recurrence or distant metastatic disease. As an example of a follow-up strategy, the one proposed by Dekkers et al.[101] is proposed: rectoscopies every six months for the first two years, then annually for the following five years, and annual CEA determination. In addition, add annual MRI or echoendoscopy and chest/abdominal CT in the first year, then at three and five years.
pT1 in the rectum, with deep submucosal invasion (>SM-1) as the only risk factor: The European ESGE guidelines also propose a more conservative approach in this case[49]: close surveillance and/or chemo-radiotherapy, without ruling out surgery, always after individualizing each case and within a multidisciplinary committee.
Conclusions and areas for improvement
With the current histological criteria, more than 70% of patients with pT1 CRC meet high-risk criteria and, therefore, with a theoretical indication for surgical rescue. But most of them will not have lymphatic metastases or residual tumor after endoscopic resection[32],[33],[37]. There is therefore a risk of overtreatment by relying exclusively on histological criteria.
There is a need to "redefine" the histological criteria, especially deep submucosal invasion and the distance to the resection margin in order to consider an R0 resection. We may see changes in this regard in clinical practice guidelines in the coming years, although prospective studies with long-term follow-up are necessary, especially in the case of patients with high-risk pT1 CRC who do not undergo surgery.
In selected cases, close clinical follow-up may be indicated instead of surgery, especially in patients with comorbidities or frail elderly. Special mention should be made of rectal pT1, where a higher risk of recurrence and lymphatic metastasis has been demonstrated, but the negative consequences of surgery in this location must also be considered.
Therefore, it is essential to develop and learn endoscopic resection techniques with a minimally invasive approach to obtain higher R0 resection rates, which will help to improve the histological evaluation of lesions, with the aim of achieving organ preservation and avoiding the dreaded adverse events of surgery (especially in the rectum).
The future lies in the development of artificial intelligence, which will improve optical endoscopic diagnosis and histological evaluation of lesions. The use of predictive models with new molecular biomarkers will also make it possible to make more precise estimates of the individual risk of each patient and facilitate the decision-making process.