
 Descargar número completo
Descargar número completo Download full issue
Download full issueCITE THIS WORK
Plaza Fernández A, Rodríguez Mateu A, Diéguez Castillo C. A “C” triad: cirrhosis and cholangitis due to caroli disease. RAPD 2024;47(3):130-132. DOI: 10.37352/2024473.6
Introduction
Caroli syndrome (CS) is a rare congenital pathology of probable autosomal recessive inheritance characterised by saccular or cystic dilatations of the intrahepatic bile ducts associated with congenital hepatic fibrosis and development of portal hypertension. A common form of presentation is recurrent cholangitis associated with hepatic abscesses as in the present case.
Clinical case
A 46-year-old woman from Romania with cirrhosis of the liver of unrelated aetiology since childhood associated with subsequent alcohol consumption, in abstinence more than one year. Previous admissions for edemoascitic decompensation and varicose ADH, carrier of TIPS. During the last year she has required five admissions following an episode of acute cholangitis with endoscopic biliary drainage and subsequent development of persistent liver abscesses/phlegmons despite multiple antibiotic therapies aimed at microbiological isolation, opting for chronic antibiotic treatment. She attended the emergency department for fever and pain in the right hypochondrium and was started on intravenous antibiotics. A follow-up CT scan showed resolution of the residual phlegmonous area and described multiple millimetric cystic liver areas.
In view of the suspicion of CD, magnetic resonance cholangiography (MR cholangiography) was performed, confirming the presence of these cystic areas which communicate with the biliary tract, giving rise to fusiform dilatations of the smaller biliary radicals located mostly towards the periphery of the liver parenchyma, compatible with CD. Finally, the patient was discharged and it was decided to evaluate the patient for liver transplantation.
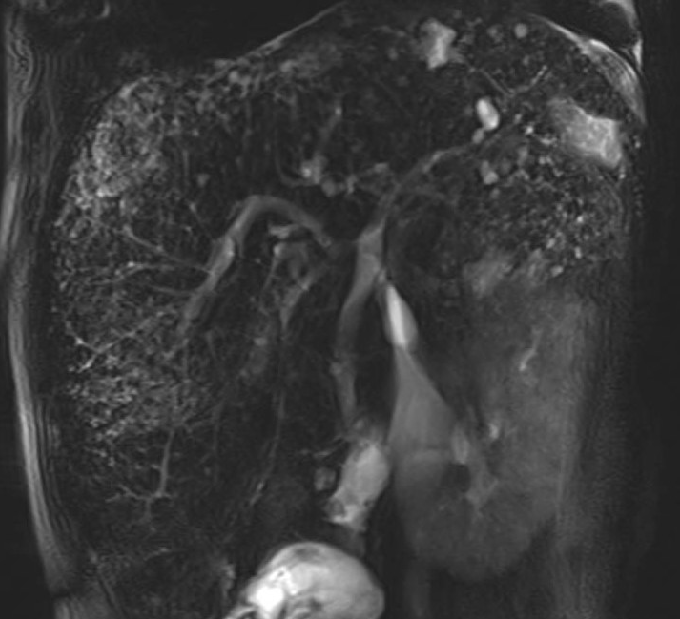
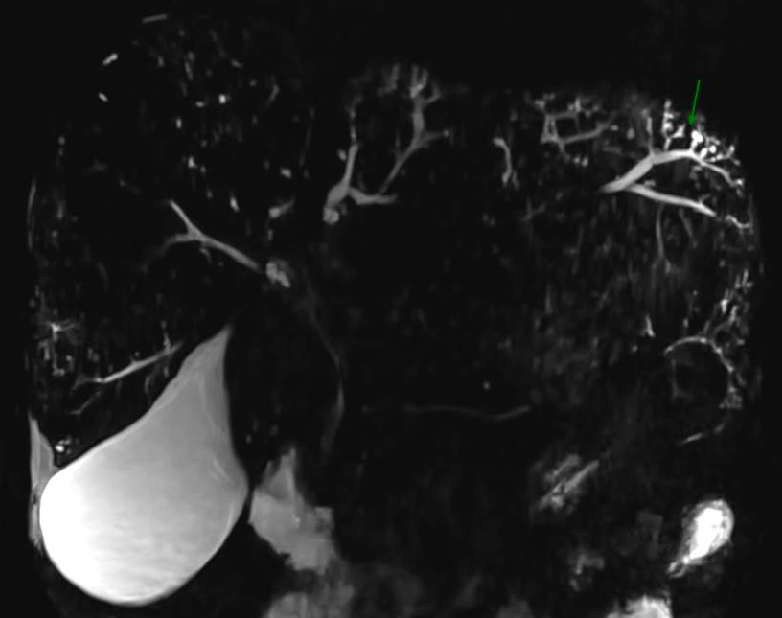
Figure 1
Cystic dilatation of the bile duct in the dome of segment VII in proximity to the intrahepatic cava.

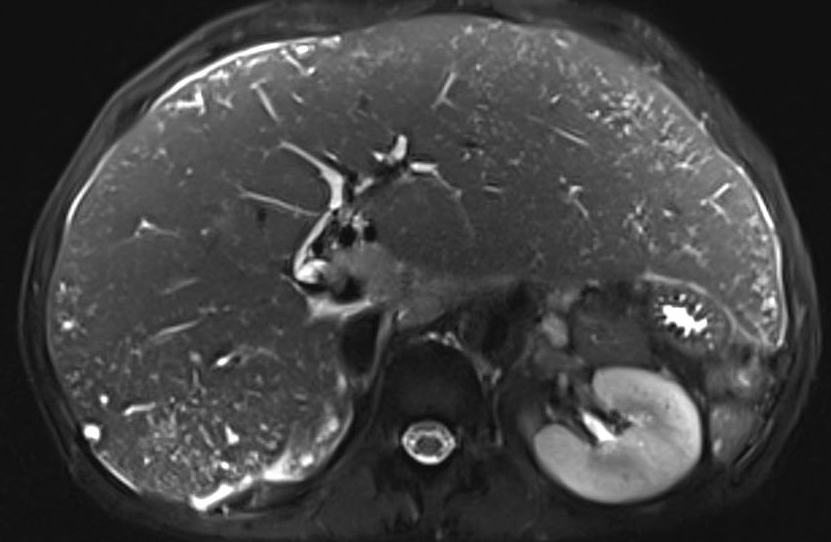
Figure 2
Axial section. Spindle-shaped dilatations of the smaller biliary radicals predominantly towards the periphery of the liver parenchyma, secondary to communication between the multiple millimetric cystic areas and the bile duct.
Discussion
CS is a congenital biliary pathology resulting from a defect in the remodelling of the ductal plate during embryogenesis. The clinical manifestations may appear during childhood or in adulthood, and are often diagnosed late.
The main symptom is recurrent abdominal pain secondary to intrahepatic stone formation. Acute cholangitis crises are also common, occurring spontaneously or after manipulation of the bile duct, with usual microbiological isolation of gram-negative germs, and often leading to the formation of liver abscesses as in the case described.
Diagnosis is mainly radiological, with MR cholangiography confirming findings of cystic areas communicating with the biliary tree and presenting saccular dilatations of monolobular or diffuse distribution. Control of the focus with antibiotic therapy is complicated, usually requiring partial lobectomy or liver transplantation depending on the extent of the disease. For the treatment of abdominal pain secondary to hepatolithiasis and mild disease, ursodeoxycholic acid at high doses has proved beneficial.
Thus, CS is a rare pathology to be taken into account in patients with liver disease of non-filial origin with recurrent episodes of acute cholangitis because of its enormous significance in the need for liver transplantation.