
 Descargar número completo
Descargar número completo Download full issue
Download full issueCITA ESTE TRABAJO
Saldaña García L, Hernández Pérez AM, Méndez Sánchez IM, López Vega MC, Fernández Moreno N, Pérez Aisa A. Profile of patients diagnosed with hydrogen-producing intestinal bacterial overgrowth and intestinal methanogenic overgrowth in a second level hospital. RAPD 2024;47(4):144-151. DOI: 10.37352/2024474.1
Abbreviations
SIBO: intestinal bacterial overgrowth.
SIBO-H: intestinal intestinal hydrogen-producing bacterial overgrowth.
IMO: intestinal methanogenic overgrowth.
OGTT: oral glucose overload breath test.
IBD: inflammatory bowel disease.
DM: diabetes mellitus.
IBS: irritable bowel syndrome.
PPIs: proton pump inhibitors.
FODMAPS: fermentable oligosaccharides, disaccharides, monosaccharides and polyols.
Introduction
The normal small intestine, has lower levels of microbial colonisation compared to the colon, when this balance is significantly disturbed it gives rise to the SIBO. This is characterised by the presence of excessive numbers of bacteria in the small intestine leading to pathological fermentation of nutrients and maldigestion of substrates that are normally fully absorbed in the small intestine, leading to symptoms resulting from excess gas production[1]. Quantitative culture of the proximal small bowel aspirate is the gold standard for objectively measuring the number of bacteria in the small intestine, with a bacterial colony count of ≥103 colony-forming units per millilitre (CFU/mL) in a duodenal/jejunal aspirate recently established as diagnostic of SIBO[2]. However, in order to be performed, the implementation of an upper endoscopy is necessary with the consequent risks of this invasive test. Therefore, a widely accepted, easy and inexpensive alternative method for the diagnosis of SIBO, based on the premise that human cells are incapable of producing hydrogen or methane, is the measurement of these gases in the breath after ingestion of a carbohydrate substrate such as glucose or lactulose[3].
The human microbiome is strongly intertwined with health and disease. In addition to bacteria, viruses and eukaryotes, numerous archaea are found in the human gastrointestinal tract and are responsible for methane production[4]. Recently, with the recognition of their role in the pathophysiology of SIBO, a new concept has been introduced, namely methanogenic intestinal overgrowth (MOI). Despite this, many aspects such as the clinical profile, the sensitivity of diagnostic tests and medical treatment, which to date has been largely empirical, remain an enigma.
In 2020, The American Journal of Gastroenterologist (AJG) published a clinical guideline on SIBO in an attempt to re-evaluate the evidence to date and propose recommendations to characterise and standardise the management of these patients in routine clinical practice[5]. The AJG concludes that most of the recommendations are weak and the evidence is of low quality and emphasises the current unmet needs in SIBO research, as well as the controversies in the field regarding the clinical profile, diagnosis and treatment of these patients. In our centre, oral glucose overload breath test (OGTT) has been routinely performed to measure hydrogen concentrations in exhaled air to diagnose hydrogen-producing bacterial overgrowth (SIBO-H) in patients with suggestive symptomatology and predisposing factors[6]. Given that up to 38% of the general population is methane fermenting[7], measurement of methane concentrations has recently been incorporated into the assessment of IMO with the aim of improving the diagnostic spectrum of this entity.
These recent changes in the diagnostic approach to this entity have motivated this study to describe the clinical-epidemiological characteristics of patients with SIBO-H and IMO and to analyse the differences between the two groups.
Material and methods
An observational, retrospective and single-centre, retrospective study was conducted where adult patients seen in the Digestive System consultations of the Costa del Sol University Hospital were included, from november 2022 to june 2023, who presented symptoms suggestive of SIBO, in whom OGTT (75 g of glucose in 200 mL of water) had been performed measuring hydrogen and methane concentrations in exhaled air to assess SIBO-H and IMO according to standard clinical practice.
The selected patients had a symptom profile suggestive of SIBO such as abdominal pain, bloating, gas, distension, flatulence, constipation or diarrhoea, as well as risk factors for SIBO such as anatomical bowel or motor complex disorders.
Patients were given recommendations to follow in the 48 hours prior to the test. These included a minimum fasting period of 12 hours, not smoking from the night before, avoiding fermentable carbohydrates and dietary fibres for at least 24 hours beforehand. They were also advised not to exercise beforehand and to brush their teeth in the morning with antiseptic solution. The test was performed at least four weeks after taking antibiotics and two weeks after colon cleansing for endoscopic or surgical procedures.
Initially, a basal alveolar sample was taken which had to be less than 10 ppm hydrogen. Values between 10 and 20 ppm pointed to incomplete fasting before the test or slow digesting food intake the day before the test, so they were recalled for a repeat test after specific re-education.
For the breath test, 75 gr of glucose diluted in 200 mL of water was used as substrate, using a diagnostic kit with sample collection tubes supplied by ISOMED PHARMA for breath measurement and sampling. The basal sample was collected and after dilution, alveolar samples were taken with forced expiration at 15-minute intervals for 120 minutes. Symptoms during the test were recorded. Attention was paid to breath sampling, storage and stability of the sample and to the specific instructions of the manufacturer, in order to ensure the accuracy of the test.
The results were submitted for combined hydrogen and methane reading with QuinTron at the ISOMED PHARMA reference laboratory.
The test was considered negative when no pathological increase in hydrogen or methane concentrations in exhaled air above baseline was identified during 120 minutes. An increase in exhaled air hydrogen concentration of 20 ppm above baseline at 90 minutes of testing was considered to be compatible with SIBO-H. An increase of 10 ppm above baseline in exhaled air methane concentration at any time during the test (120 minutes) was considered compatible with IMO.
The primary outcome variable was SIBO phenotype (SIBO-H or IMO). Covariates were age, sex, presence of symptoms leading to the test and symptoms during the test, predisposing factors, medical treatment used, subsequent follow-up and the performance of a second OGTT to assess the decrease in hydrogen or methane production after treatment. A comparison of both groups was made between the variables studied.Student's t-test was used for quantitative variables and Chi-Square for qualitative variables. A value of p<0.05 was considered statistically significant.
Results
We analysed 116 patients with symptomatology suggestive of intestinal bacterial overgrowth in whom OGTT had been performed to evaluate SIBO-H and IMO, of whom 26 were eligible with positive hydrogen or methane result (22.41%). SIBO-H was diagnosed in 50% (13) and IMO in 50% (13) (Table 1), with a median age of 53 and 57 years respectively (Table 2).
Table 1
Results of the oral glucose overload breath test to assess intestinal hydrogen-producing bacterial overgrowthand intestinal methanogenic overgrowth.
Table 2
Epidemiological factors associated with intestinal hydrogen-producing intestinal bacterial overgrowth and intestinal methanogenic overgrowth.
Associated risk factors were: hypothyroidism 15.4% (2) in both groups, bowel resection with anastomosis 23.1% (3) in both groups and in the case of SIBO-H, diabetes mellitus 23.1% (3). All patients older than 65 years[3] tested positive for IMO. One patient with IMO (7.7%) had irritable bowel syndrome (IBS) (Table 2).
Table 3
Treatment used in patients diagnosed with intestinal hydrogen-producing bacterial overgrowth and intestinal methanogenic overgrowth.
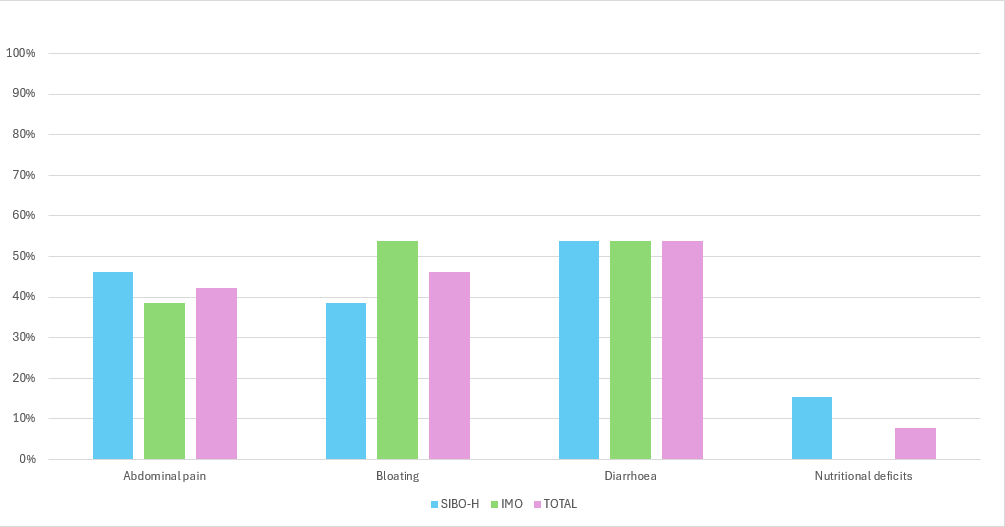
The most frequent symptom was diarrhoea 53.8% (7) in both groups. Abdominal pain was more frequent in patients with SIBO-H 46.1% (6) versus 38.5% (5) in the IMO group. For meteorism, it was more frequent in IMO patients 53.8% (7) versus 38.5% (5) in SIBO-H patients (Figure 1). No cases of constipation were identified in the studied sample. There were no statistically significant differences between the two groups for the variables studied.
Figure 1
Symptomatology associated with hydrogen-producing intestinal bacterial overgrowth and methanogenic intestinal overgrowth.
Of the 26 patients who tested positive, 17 (9 with SIBO-H and 8 with IMO) received medical treatment. The most commonly used treatment for SIBO-H was Rifaximin 88.9% (8). In IMO Rifaximin and Metronidazole 50% (4) and Rifaximin and Neomycin 37.5% (3) were used. The test was repeated with the intention to assess treatment outcome in one patient with SIBO-H and in three with IMO. The post-treatment test was negative in only one patient with IMO.
SIBO is defined by the presence of an abnormal amount of bacteria in the small intestine, which ferment carbohydrates and produce gas leading to the occurrence of symptoms such as bloating, abdominal pain, diarrhoea and constipation.
Although most patients with SIBO produce hydrogen, 30-38% are colonised with archaeal species. Archaea are anaerobic organisms that produce methane and are resistant to many systemic antibiotics. The excessive presence of archaea in the small intestine, and the symptoms resulting from nutrient fermentation, is known as IMO; a newly recognised entity within the SIBO profile. However, it is unclear whether IMO is distinguished by a distinctive set of gastrointestinal symptoms and predisposing conditions[7].
Culture of jejunal aspirate obtained by upper gastrointestinal endoscopy is the gold standard for the diagnosis of SIBO, with a bacterial colony count of ≥103 CFU/mL being considered diagnostic[8]. Breath tests are performed in daily clinical practice for the diagnosis of many common conditions of the gastrointestinal tract such as carbohydrate maldigestion, oro-cecal transit dysfunction or disturbances and SIBO. Substrates such as glucose, lactulose, fructose, sorbitol, sucrose and inulin can be used. The rationale of the breath test is that both hydrogen and methane are produced exclusively through microbial fermentation in the gut. Intestinal microorganisms readily digest carbohydrates, resulting in the production of these gases, which then diffuse into the abdominal venous circulation and are transported to the lungs, where they can be detected in the exhaled breath[3]. Quantitative measurement of hydrogen and methane in exhaled air after ingestion of a quantity of carbohydrates is an indirect method and a non-invasive, easy and readily available test recommended by scientific evidence to assess SIBO as an alternative to jejunal aspirate[5]. The sensitivity of the lactulose oral overload breath test has ranged from 31% to 68% and the specificity has ranged from 44% to 100%, while the sensitivity of glucose oral overload breath tests has ranged from 20% to 93% and the specificity from 30% to 86% compared to small bowel aspirate cultures[5]. The lactulose-overloaded breath test results in a higher number of false positives, which is why glucose is considered the substrate of choice to administer as performed in our study[1].
In the evidence reviewed, the prevalence of SIBO is around 30%[7] vs. 22.41% in our study. Regarding IMO, a prevalence of up to 38.8% has been reported in patients with SIBO[7] vs. 50% in our study. In accordance with the literature, we found a predominance of SIBO in the female sex (69.2%) and the mean age was 53 years, similar to that described in other studies[7]. It is striking that all patients in the sample older than 65 years were diagnosed with IMO, which supports the positive relationship between age and colonisation by methanogenic archaea[7].
Regarding predisposing factors, although IBS is one of the conditions most commonly assessed as being linked to SIBO[5],[9], in this study it was present in only 7.7% of patients with IMO. Mechanical anatomical disorders of the small bowel[6] and motility disorders have been linked to abnormal accumulation of bacteria in the small bowel[10], both of which were present in the patients under study with a predominance of intestinal resections with anastomosis and hypothyroidism in both SIBO-H and IMO patients. Several studies suggest that 50% of patients with thyroid dysfunction have SIBO[11]. Diabetes mellitus has been shown to be significantly more prevalent in patients with SIBO (12)[7], however, in our study it was present in only 25% of patients with IMO and in no SIBO-H patients.
It has been postulated that treatment with PPIs, with the consequent decrease in gastric acidity, could be a risk factor for the development of SIBO[13]; however, the scientific evidence in this regard is contradictory[5]. In our study, 7.7% of patients with SIBO-H and 15.4% of patients with IMO were treated with PPIs, which is to be expected given the high consumption of PPIs in the general population.
In terms of symptomatology, abdominal pain with bloating, diarrhoea and meteorism are the most commonly described symptoms in the scientific evidence[5]. Diarrhoea has been most commonly associated with SIBO-H[14], however, in our study no differences in symptomatology were found between patients with SIBO-H and IMO.
Multiple studies have shown that methane-positive OGTT is related to constipation and that the level of methane in exhaled air is proportional to the degree of constipation[14],[15]. However, none of the patients diagnosed with OMI in this study had constipation.
Evidence suggests antibiotic treatment in patients with SIBO to eradicate the overgrowth of microorganisms in the small intestine[5]. In the case of SIBO-H, Rifaximin, although lacking in high quality studies, is supported by the most evidence[16] and has been the most commonly used monotherapy in the patients with SIBO-H under study. In the case of patients with IMO, evidence suggests that the combination of Rifaximin and Neomycin is able to reduce methane to undetectable levels[17]. In our study, 37.5% of patients with IMO received Rifaximin and Neomycin in combination.
There are other non-drug treatments used in patients with SIBO with little evidence such as the use of probiotics[18], low FODMAPS (fermentable oligosaccharides, disaccharides, monosaccharides and polyols) diet[19] and herbal products[20] which were not used in the patients under study.
The limitations of our study include its retrospective design, which prevents us from determining causality, as this requires prospective longitudinal studies. Secondly, the small sample size may have influenced the absence of significant results. On the other hand, not all patients diagnosed and treated had been re-evaluated at the time of this study, largely due to the time lag, which prevented us from assessing symptomatic improvement after treatment or breath test negativities.
As strengths, our study analyses the characteristics of patients with IMO; an entity little studied to date and with many enigmas in terms of clinical profile, diagnosis and management.
Conclusions
In view of the results obtained in the present study SIBO is a relatively frequent entity in our study (22.41%). The routine implementation of measurement of hydrogen and methane concentrations in exhaled air has allowed the diagnosis of IMO in 50% of patients with SIBO; however, no significant differences have been found to demonstrate distinctive features of SIBO-H and IMO in terms of epidemiological factors, symptomatology, diagnosis or treatment.