
 Descargar número completo
Descargar número completo Download full issue
Download full issueCITA ESTE TRABAJO
Calvo Bernal MM, Sánchez Moreno S, Cuello Entrena E, Hallouch Toutouh S. The pancreas through the skin: pancreatic panniculitis, importance of early diagnosis. RAPD 2024;47(4):163-165. DOI: 10.37352/2024474.5
Introduction
Pancreatic panniculitis (PP) is a rare cutaneous manifestation of pancreatic processes. Its clinical presentation is indistinguishable from other types of panniculitis, so differential diagnosis with other entities is essential. The importance of its early detection lies in the fact that in up to half of the cases its appearance precedes the underlying pancreatic disease, whether benign or malignant, and it carries a worse prognosis.
Clinical case
We present the case of a 74-year-old female patient with a history of hypertension, diabetes and chronic lymphocytic leukaemia on treatment with ibrutinib, who was admitted to the hospital ward with a diagnosis of acute pancreatitis (AP) after presenting with clinical symptoms of epigastralgia associated with vomiting of four days' duration and a blood test showing hyperamylasaemia of 3,040 U/L.
On the third day of admission, the patient presented poor pain control and respiratory distress with bilateral pleural effusion. Laboratory tests showed deterioration of renal function and elevated acute phase reactants (CRP 46 mg/dL) requiring transfer to the ICU. An abdominal CT scan was performed showing AP and necrosis <30%, with a persistent torpid evolution, so a CT scan was requested one week later showing extensive peripancreatic necrosis and a 12 cm collection (Figure 1).
Figure 1
Abdominal CT scan. There is an increased density of peripancreatic fat with peripheral enhancement, in relation to a collection with necrotic tissue up to 12 cm in the major axis.

On admission, the patient presented violaceous nodular lesions on both lower limbs, painful on palpation (Figure 2), assessed by Dermatology, which performed a subcutaneous biopsy (Figure 3) with findings of panniculitis.

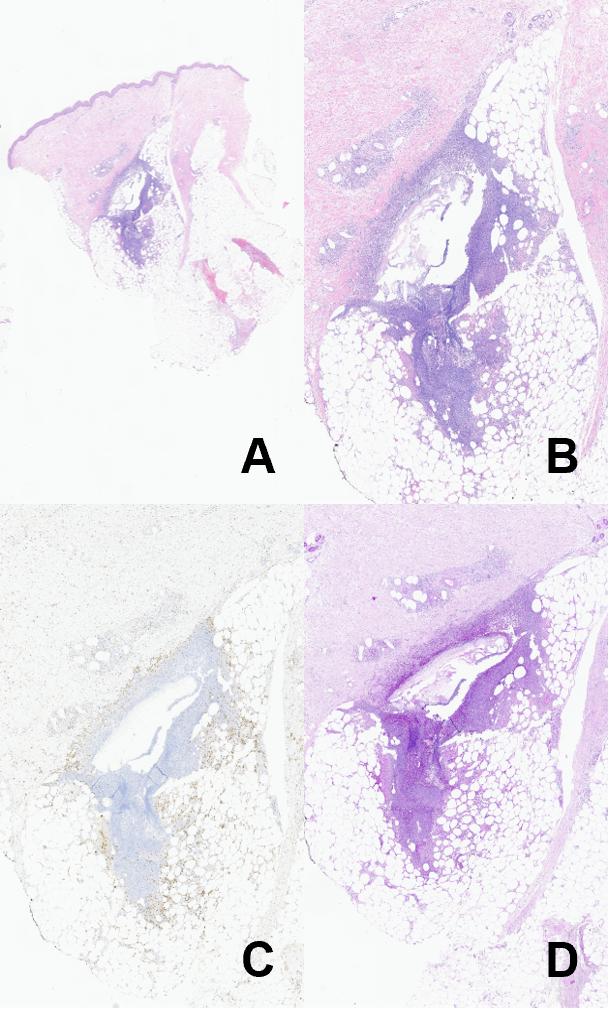
Figure 3
Pathological anatomy. A and B. Haematoxylin-eosin stain (1x and 4x). There is an area of tissue necrosis with predominantly lobular abscessation at the junction of the deep dermis with the adipose panniculus. C. CD68 stain showing the presence of a chronic inflammatory infiltrate with abundant foamy macrophages. D. PAS+ stain (4x) in the centre of the necrotic area.
The patient's evolution was torpid, with progressive worsening, finally presenting multiorgan failure and exitus after three weeks of hospitalisation.
Discussion
PP or enzymatic necrosis of subcutaneous fat was first described by Chiari in 1883 in patients with acute pancreatitis. It is a rare complication of pancreatic processes, with a prevalence of 3%[1],[2] and usually appears between the fourth and sixth decade of life, with a higher prevalence in males (male to female ratio 5:1).
It manifests as erythematous or purplish nodules, painful on palpation, which may spontaneously ulcerate and emit an oily material. They usually affect the lower limbs, but may also extend to the buttocks, trunk, arms and scalp. It may be associated with systemic manifestations such as fever, abdominal pain, polyarthrosis and less frequently, ascites or pleural effusion[3]-[6]. Its clinical course parallels that of the underlying condition and has been associated with both benign pancreatic diseases (most frequently in acute pancreatitis) and malignant diseases[2],[7].
The dermal lesions are indistinguishable from other panniculitis, requiring differential diagnosis with other panniculitides, such as erythema nodosum, lupus panniculitis, sarcoidosis-related panniculitis and erythema induratum of Bazin or nodular vasculitis[1].
Diagnosis is confirmed by subcutaneous biopsy. The histopathological picture consists of lobular panniculitis with the presence of necrosis of the subcutaneous adipose tissue due to its digestion by pancreatic enzymes. Characteristic, although not pathognomonic, is the presence of necrotic adipocytes known as ‘ghost cells’[2],[7].
Treatment of PP is directed at the underlying pancreatic disease. Subcutaneous signs usually subside within 15-30 days after onset. Some studies suggest the use of somatostatin analogues such as octreotide to alleviate symptoms due to their role as inhibitors of pancreatic secretion, although experience with these drugs is limited[1],[7]. The prognosis is poor in cases associated with pancreatic carcinoma.
The clinical importance of this condition derives from the fact that skin lesions usually precede clinical manifestations of pancreatic involvement in up to 45% of cases, so that the appearance of this entity obliges us to rule out pancreatic disease, even in asymptomatic patients[7]. In the case of known pancreatic patients, the appearance of this dermatosis may indicate a flare-up of a chronic condition, casting a shadow over the prognosis.