
 Descargar número completo
Descargar número completo Download full issue
Download full issueCITA ESTE TRABAJO
Moreno Barrueco M, Bailón Gaona MC, Gijón Vilanova R, Berdugo Hurtado F, García Robles A. Enteropathy-associated T-cell lymphoma: from indolent to aggressive. RAPD 2024;47(5):184-186. DOI: 10.37352/2024475.2
Introduction
The gastrointestinal tract is a common site for the seat of extranodal lymphomas. Primary gastrointestinal lymphomas are predominantly type B, and T-cell neoplasms are rare and account for 13-15% of gastrointestinal lymphomas. Enteropathy-associated T-cell lymphoma (EATL) is a rare neoplasm, accounting for <5% of peripheral T-cell lymphomas and is a frequent complication of celiac disease.
Clinical case
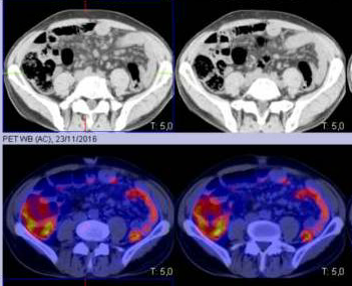
A 59-year-old man with a history of incidental finding in 2016 of mesenteric adenopathies by abdominal CT in the context of epigastralgia and constitutional symptoms, subsequently studied by haematology by PET-CT (Figure 1), which describes the presence of retroperitoneal and mesenteric non-catching adenopathies, without being able to rule out the possibility of indolent mature lymphoid neoplastic involvement; An excisional biopsy was therefore performed on one of the lymph nodes, in which the anatomopathologists described mild lymphoid hyperplasia, with no signs of malignancy. Subsequently, he was diagnosed with coeliac disease in April 2022 due to a study of hypertransaminasemia with positive transglutaminase antibodies and HLA DQ2 +. An upper gastrointestinal endoscopy (EGD) and duodenal biopsies were performed to confirm the diagnosis, describing partial villous flattening (Marsh type 3a lesions) and intraepithelial lymphocytosis (more than 6 CD3+ lymphocytes per 20); with a good response to the gluten-free diet. In May 2022, she was admitted to neurology in May 2022 for the debut of seronegative myasthenia gravis, with treatment commencing in December 2022 with azathioprine 1mg/kg due to persistent diplopia.
Figura 1
PET-CT scan performed in 2016 described the presence of retroperitoneal and mesenteric non-catching adenopathies, without being able to rule out the possibility of indolent mature lymphoid neoplastic involvement.
He was admitted to our department in June 2023 due to afternoon fever, watery diarrhoea and loss of more than 15 kg in the last 3 months. After verifying good adherence to the gluten-free diet, a new EDA was performed with biopsies that described intense villous atrophy and CD3+ intraepithelial lymphocytosis, which in numerous points was greater than 100 lymphocytes per 100 enterocytes and on average far exceeded 50 lymphocytes per 100 enterocytes, as well as the presence of intense superficial plasmacytosis together with crypt hypertrophy. Immunophenotypically, loss of CD8- and clonal rearrangement for the TCR gamma gene, probably related to refractory celiac disease type II.
The study was completed with capsule endoscopy with the finding of multiple ulcerated areas at the level of the jejunum with surrounding thickening (Figure 2). Given the torpid clinical course, with persistent diarrhoea, fever and clear signs of malnutrition, as well as the findings previously described in imaging tests, a repeat PET-CT scan was performed to re-evaluate the lymphadenopathies previously studied, with the latter showing hypermetabolic supra- and infra-diaphragmatic lymphadenopathies suggestive of a neoplastic process (Figure 3).
Figura 2
Endoscopic capsule images showing multiple ulcerated and thickened surrounding areas at the level of the jejunum.

Figura 3
PET-CT scan for re-evaluation of previously studied adenopathies with the finding of hypermetabolic supra and infra diaphragmatic adenopathies suggestive of a neoplastic process.

The patient suffered an abrupt clinical and analytical deterioration in the following 48 hours with signs of liver failure and possible associated haemophagocytosis, and so the haematology department was informed of the possibility of marrow infiltration by the neoplastic process, and a bone marrow biopsy was performed with the result of infiltration by a CD30+ large T-cell lymphoproliferative process, together with macrophages with signs of haemophagocytosis. Empirical treatment with chemotherapy (mini-CHOP) was started urgently without success, and the patient died in the following days due to acute liver failure.
Discussion
Enteropathy-associated T-cell lymphoma (EATL) arises from malignant transformation of intestinal intraepithelial lymphocytes and is the most common neoplastic complication of celiac disease. It slightly predominates in males (54%), mainly older than 50 years. It is uncommon in patients diagnosed early or with long-standing coeliac disease, and may even present as the initial form of the disease. Other factors associated with its occurrence are viral infection and the presence of the HLA-DQ2 haplotype. Although there are sporadic cases, refractory coeliac disease (RCD) type II is strongly associated as a preneoplastic process.
90% of cases of EATL are located in the small intestine, mainly in the jejunum, where multiple ulcers are often found. They can spread beyond the gastrointestinal tract, the most relevant locations being abdominal lymph nodes (35%), bone marrow (3-18%), pulmonary and mediastinal lymph nodes (5-16%).
Clinically, it may present with symptoms similar to RCD, such as diarrhoea, abdominal pain, weight loss and hypoalbuminaemia. Therefore, computed tomography (CT), PET-CT and capsule endoscopic imaging are useful to identify the progression of RCD to LTLE. It may also manifest with vomiting due to intestinal obstruction, intestinal haemorrhage and intestinal perforation in up to 50% of patients. Haemophagocytic syndrome is reported in 16-40% of cases.
Information on the pathogenic mechanisms is limited due to its rarity, although it has been suggested that an inflammatory microenvironment, especially mediated by the JAK-STAT pathway, might have a high impact on its lymphomagenesis.
Early diagnosis requires a high degree of suspicion and careful examination of intestinal biopsies. Morphologically, it is characterised by pleomorphic cytology, so immunohistochemistry is crucial for diagnosis. Neoplastic cells are usually CD3 + CD7 +, CD103 + cells, TCRβ +/-, CD4-, CD8- and CD5-, with primary expression of CD30 and negativity for CD56. Genetic susceptibility has been demonstrated in patients with HLA-DQ2.5 homozygosity, observed in up to 53.3% of patients with EATL.
The prognosis is poor, with survival rates of around 1 and 5 years. There is no standardised treatment for this aggressive lymphoma. Surgery and chemotherapy (CHOP regimen) are considered treatment options, but EATL tends to be refractory to these therapies, with an overall median survival of 6 months despite their application.