
 Descargar número completo
Descargar número completo Download full issue
Download full issueCITA ESTE TRABAJO
Campos Gonzaga L, Aguilar Martínez JC, Moreno García A. From caustic soda ingestion to feeding jejunostomy. RAPD 2024;47(5):190-191. DOI: 10.37352/2024475.4
Introducción
Caustic ingestion often leads to high morbidity and mortality, ranging from mild cases without lesions to severe cases with total necrosis of the upper digestive tract. The intensity and location of the lesions depend on several factors, the most important being the type of caustic (alkalis have greater penetrating power).
Clinical case
32-year-old woman with a personal history of anxious-depressive syndrome under follow-up since 2019 by the Mental Health unit with several self-harm attempts. In July 2023 she made an autolytic attempt due to caustic ingestion, showing caustic oesophagitis Zargar grade IIIb (Figure 1), caustic gastritis Zargar grade IIIb, caustic duodenitis Zargar grade IIIb (Figure 2) and caustic lesions in Killian's mouth on upper gastrointestinal endoscopy (EGD), performed at 24 hours, and caustic lesions in Killian's dehishence. She was admitted to the ICU for 7 days and then to the ward with parenteral nutrition for 3 weeks. Prior to discharge, tolerance to liquids and triturates was started with a good response. In the following months the patient visited the emergency department on several occasions, presenting in September 2023 with marked intolerance to solids and liquids that caused vomiting and made it impossible to take oral treatment.
Figura 1
From the cervical oesophagus to the middle oesophagus, the mucosa shows oedema, with superficial fibrinous ulcerations with diffuse exudate occupying the entire oesophageal circumference. The lesions become more intense in the distal oesophagus, with the oesophagus acquiring a blackish-ischaemic appearance, with deep ulcerations with a dirty bottom that occupy the entire oesophageal circumference.

Figura 2
Gastric cavity with black mucosa with diffuse mucous exudate, with more expressive lesions in the antral region with deep ulcers with a dirty bottom. The mucosa of the duodenal bulb and second portion shows large diffuse ulcerations, confluent at some points.

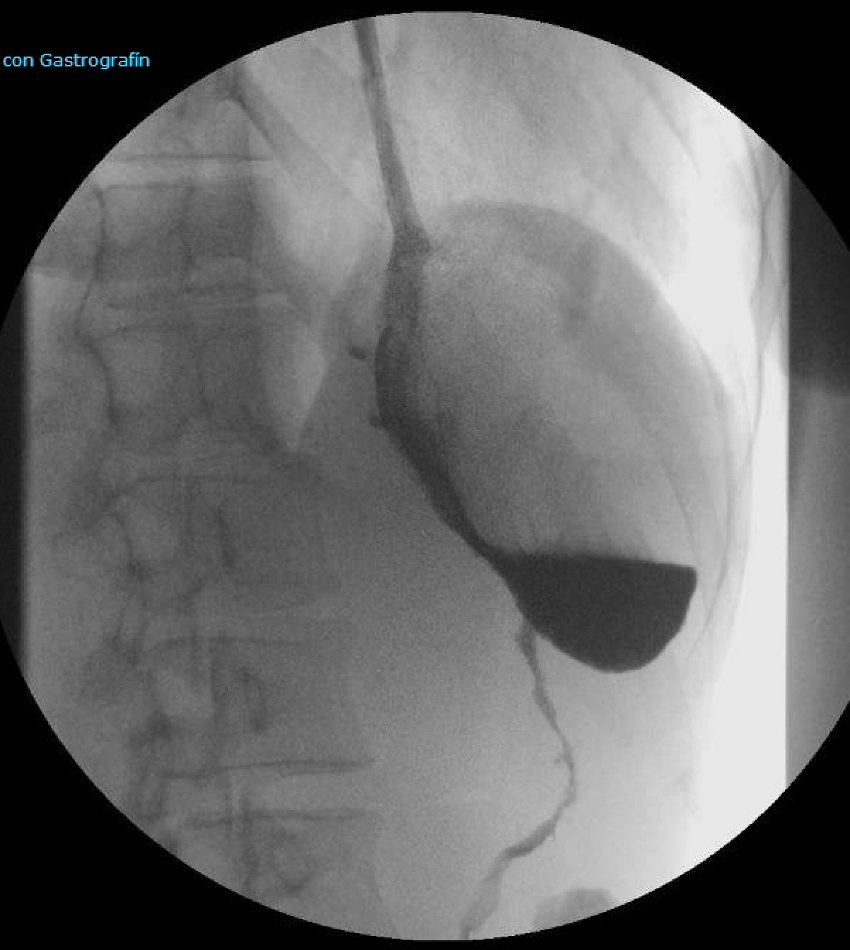
A barium study performed during follow-up showed diffuse stenosis in the middle and lower thirds of the oesophagus and extensive and marked stenosis of the body, gastric antrum and duodenal bulb (Figure 3). For this reason, IC was referred to surgery, proposing a feeding jejunostomy, after performing an EGD, which showed impassable oesophageal stricture 30 cms from the dental arch.
Figura 3
Oesophageal stricture with a marked decrease in diameter, with a luminal diameter of 4 mm. There is extensive and marked stenosis of the body, gastric antrum and duodenal bulb, with filiform passage of contrast, with marked irregularity of the contour, compatible with marked thickening of folds and ulcerations. Scarce passage of contrast into the duodenal frame.
Discussion
The management of patients with caustic ingestion lesions is complex, posing a real therapeutic challenge, not only in the acute phase but mainly in the late phase. Strictures usually appear from the second to third week, and may manifest themselves clinically after months or years, and the risk of developing squamous cell carcinoma is increased.
Endoscopic dilatation or prosthesis placement can be considered in localised and short strictures, but in cases such as our patient's, coordination between the surgical and medical teams is required to obtain the best results.[1],[2].