
 Descargar número completo
Descargar número completo Download full issue
Download full issueCITA ESTE TRABAJO
Lancho Muñoz A, Ortega Suazo EJ, García Aragon F, Redondo Cerezo E. Chronic mesenteric ischemia, an undervalued cause of constitucional syndrome. RAPD 2024;47(6):226-229. DOI: 10.37352/2024476.6
Introduction
Chronic mesenteric ischaemia (CMI) is an uncommon digestive pathology in clinical practice, caused by a decrease in flow, due to low output or the presence of stenosis, in the main mesenteric vessels[1], the anatomy of which is detailed in table 1.
Tabla 1
Irrigación visceral de cada una de las estructuras vasculares arteriales que constituye el territorio vascular mesentérico.
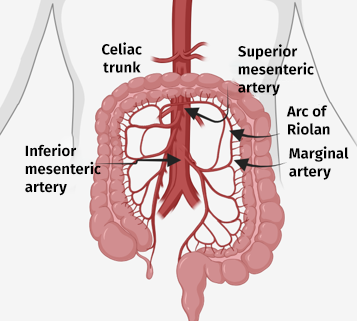
Clinically, less than 2% of patients present with the characteristic triad of abdominal pain, sitophobia and unintentional weight loss. This lack of symptoms is due to the fact that the bowel is protected from ischaemia by the existence of multiple collaterals between its main vessels, such as the pancreatoduodenal artery between the CA and the SMA or the marginal artery and the arc of Riolan between the SMA and the IMA (Figure 1). However, an increase in incidence has been observed over the last decade, secondary to population ageing and the increased prevalence of cardiovascular risk factors such as hypertension, diabetes or obesity, which is why it is increasingly diagnosed in gastroenterology consultations or endoscopy units[2].
The characteristic symptoms of CMI are frequently observed in patients with constitutional syndrome, and CMI and other non-neoplastic digestive pathologies, such as peptic disease or chronic pancreatitis, should be included in the differential diagnosis[3]. All of these pathologies, including CMI, are associated with a high morbidity and mortality rate, which is directly proportional to the delay in diagnosis and initiation of therapeutic measures. Initially, conservative management with hygienic-dietary measures and control of cardiovascular risk factors is chosen, opting for a surgical approach in the case of symptomatic patients or those with significant vascular involvement[4].
Clinical case
We present the case of a 65-year-old patient with several cardiovascular risk factors, including arterial hypertension, dyslipidaemia, type II diabetes and active smoking. He had a history of chronic ischaemia in the lower limbs secondary to generalised atherosclerotic disease, and was being treated with cilostazol and pentoxifylline.
The patient came to the outpatient department of the Digestive System, referred from Primary Care, due to abdominal pain in the mesogastrium, predominantly postprandial, together with hyporexia and weight loss of up to 20 kg in the last three months. Laboratory tests showed hypoproteinemia (6 g/dl) with hypoalbuminemia (2.8 g/dl) and slight alteration of the liver profile (GOT 48 U/L, GPT 58 U/L, GGT 188 U/L, FA 91 U/L) with no other significant alterations.
Given the existence of alarm symptoms, it was decided to perform a complete endoscopic study with gastroscopy and colonoscopy. In this study, patchy areas of erythema and whitish mucosa were observed together with fibrinous ulcers-erosions, some of them excavated, with congestive edges, suggesting an ischaemic origin. They are mainly located in the distal gastric body, gastric antrum, duodenum and ascending colon (Figures 2-5). Histological study was compatible with chronic inflammatory infiltrate without signs of intestinal metaplasia and lymphoplasmacytic colitis in the proximal colon samples. Given the unspecificity of the histological findings and the high suspicion of an underlying ischaemic disorder, AngioCT was requested to complete the aetiological study.
Figure 2
Distal gastric mucosa at its junction with gastric antrum with patchy areas of whitish mucosa more marked towards the lesser curvature and antrum that appear ischaemic in nature visualised with white light (left) and with NBI light (right).

Figure 3
Retro-vision image showing involvement of the distal gastric body, with respect for the fornix and proximal gastric body.
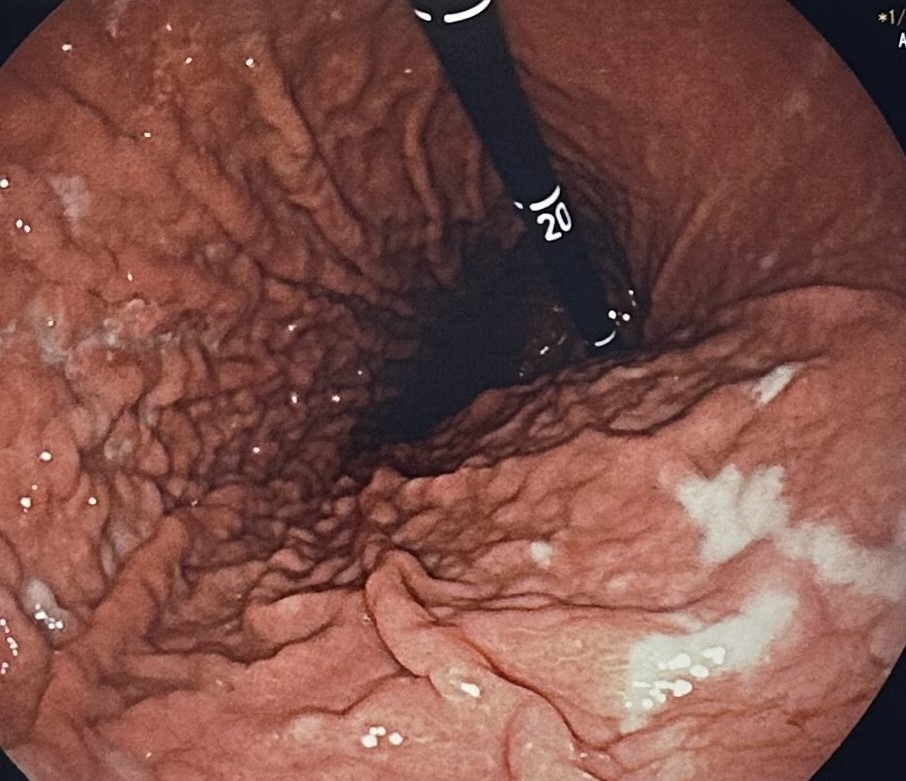
Figure 4
Second duodenal portion with patchy areas of erythema and areas of whitish mucosa, with isolated fibrinous ulcer-erosions.

Figure 5
Angio-CT reconstruction with critical stenosis at the origin of the celiac trunk and proximal occlusion of the superior mesenteric artery with filiform filling of the distal arteries.

A few days after the assessment in the consultation room, the patient came to the emergency department with severe abdominal pain and postprandial vomiting of food, with no other symptoms of interest. Examination revealed generalised pain on palpation with no signs of peritonism. An urgent abdominal CT scan showed critical stenosis at the origin of the celiac trunk with filiform filling of distal arteries and complete proximal occlusion of the superior mesenteric artery with signs of distal repermeabilisation by collaterals (a finding that suggests chronic ischaemia), both vascular occlusions caused by atheromatous plaques (Figure 6). Secondary signs of hepatic and splenic hypoperfusion are observed, without signs of intestinal loops suffering.
Figura 6
Proximal ascending colon with patchy areas of whitish mucosa and some isolated fibrinous erosions, more marked in the ileocaecal valve and cecum.

The patient was admitted and initially opted for endovascular surgical treatment with the intention of recanalising the superior mesenteric artery, which failed, with persistent postprandial abdominal symptoms. Finally, it was decided to recanalise the superior mesenteric artery by means of an aorto-mesenteric bypass, and the patient subsequently showed a slight clinical improvement.
Currently, the patient continues to be followed up by the Angiology and Vascular Surgery Department. However, given that he continues to smoke, postprandial symptoms have reappeared, together with worsening of the paraesthesias in the lower limbs.
Discussion
Chronic mesenteric ischaemia (CMI) is an underestimated digestive pathology, the late diagnosis of which is associated with an increased risk of disability and mortality. CMI occurs due to occlusive or non-occlusive causes, and the overall prevalence is unknown. In post-mortem forensic series, a prevalence of 6-29% is estimated, exceeding 67% in series of patients over 80 years of age. However, less than 2% of patients with critical stenosis of the mesenteric vessels will present with symptoms as the intestinal vasculature is characterised by collateral circulation[2]. Chronic occlusive mesenteric ischaemia may be secondary to atherosclerosis, compression of the arcuate ligament of the diaphragm, fibrodysplasia, as well as, other rare causes, such as vasculitis or thrombotic disease. Arteriosclerosis is the most common aetiology, being characteristic in women and associated with cardiovascular risk factors such as smoking, hypertension, diabetes, dyslipidaemia or family history of cardiovascular disease[4].
The most characteristic symptom of CMI is the onset of predominantly postprandial abdominal pain, starting 15-30 min after ingestion and lasting 2-4 hours (74-100% of cases). As a result, 90% of patients eventually develop a phobia of eating, reducing the frequency and quantity of their meals. Secondarily, involuntary weight loss of up to 15 kg occurs (61-94% of cases), thus completing the characteristic clinical triad: predominantly postprandial abdominal pain, sitophobia and weight loss[5]. Thus, CMI can easily be confused with a constitutional syndrome, also known as asthenia-anorexia-cachexia syndrome, for which the diagnostic criterion is a loss of at least 5% of body weight for at least 6 months[6]. Although it is generally accepted that, a priori, a neoplastic process underlies every constitutional syndrome, we must not forget other clinical entities such as non-neoplastic digestive diseases, especially CMI.
There are multiple non-standardised diagnostic algorithms that recommend imaging tests (abdominal ultrasound or abdominal CT) and/or endoscopic techniques in the presence of a constitutional syndrome, in order to avoid under-diagnosing digestive causes of neoplastic or non-neoplastic origin. The characteristic endoscopic findings of CMI are oedema (35%), erythema (42%), mucosal atrophy and erosions or ulcers (60-80%); and they usually show continuous involvement, depending on the vascular territory affected[2].
Treatment of early-stage CMI includes control of cardiovascular risk factors and lifestyle modification, especially smoking cessation. However, when symptoms appear, a surgical approach using endovascular or open procedures is recommended[1],[2].
In conclusion, CMI is an infrequent pathology with a high percentage of asymptomatic patients and whose clinical presentation resembles constitutional syndrome, we should include it in the differential diagnosis of all patients with involuntary weight loss, especially if there are added cardiovascular risk factors. On the other hand, despite the lack of specificity of the endoscopic and histological findings, endoscopists should consider it especially if these findings are limited to a specific vascular territory, as was the case in our patient, and when other more frequent causes such as neoplasms, H. pylori infection or consumption of non-steroidal anti-inflammatory drugs have been ruled out. High clinical suspicion and endoscopic findings were crucial in this case, and complications and high morbidity and mortality secondary to diagnostic delay could be avoided.