
 Descargar número completo
Descargar número completo Download full issue
Download full issueCITE THIS WORK
Garrido Gallardo A, Briceño Delgado J, Carrillo Cubero B, Lombardo Galera S. Concomitant vascular compressive syndromes: are they all described? About a case of recurrent lower gastrointestinal bleeding. RAPD 2025;48(1):27-30. DOI: 10.37352/2025481.3
Introduction
Vascular compressive syndromes consist of the entrapment of a vessel by another structure in a small anatomical space. They are rare and encompass many syndromes, some of which are not well known. Most of the time they appear incidentally, but they can be symptomatic and even require endovascular or surgical treatment, which is why it is important to be aware of them. In addition, concurrence of several syndromes has been described in the same patient without being able to determine a clear relationship between them.
Case description
A 29-year-old woman was brought to the emergency department for melaenic stools of 24 hours' duration, associated with syncope. The patient reported feeling asthenia and weakness in the last few days, with similar intermittent, self-limiting symptoms.
On examination, she was in regular general condition, with skin pallor and melena. Blood pressure 90/45 mmHg, heart rate 98 bpm. Blood tests showed haemoglobin 6.2 g/dL and haematocrit 18.8%.
As history, iron deficiency anaemia since childhood with transfusion requirements on several occasions, for which she was studied by paediatrics, internal medicine and haematology, without any diagnosis, and a body mass index (BMI) of 17.9 kg/m2. She underwent normal upper and lower gastrointestinal endoscopy, enteroresonance and video capsule, with no findings of interest.
In May 2023, a double balloon enteroscopy was performed in another centre, describing a jejunal varix.
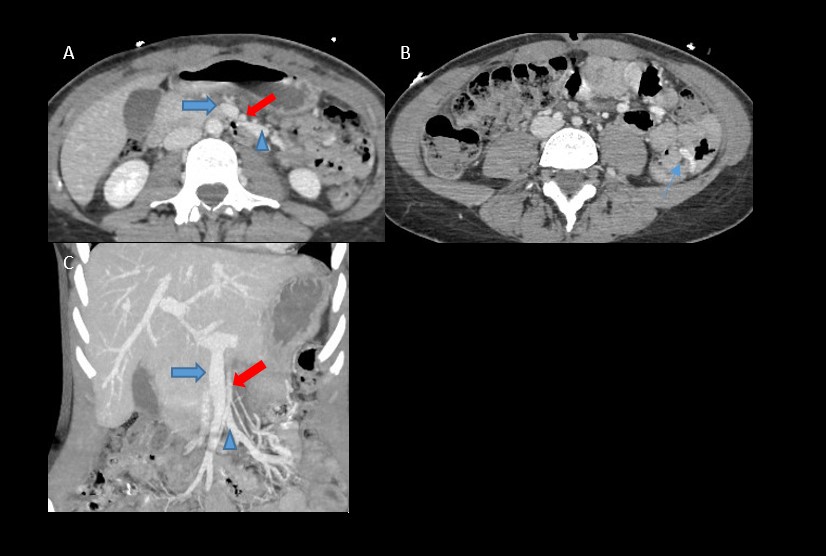
Given the patient's condition and clinical symptoms, an urgent abdominal CT angiography was requested (without contrast and with contrast in the arterial and venous phases). No active bleeding was observed in the study, but submucosal jejunal varices of significant size secondary to stenosis of the main branch of the superior mesenteric vein (SMV) just posterior to the truncal bifurcation, due to compression between the superior mesenteric artery (SMA) and the third duodenal portion (Figure 1).
Figure 1
A and B Axial CT sections of the abdomen with venous phase contrast, C Coronal section, SMA indicated with thick red arrow, SMV with thick blue arrow and with blue arrowhead jejunal vein. A. Stenosis of SMV due to compression with the MSA and subsequent dilatation; B. Varicose vein in the jejunal submucosa (blue arrow); C. Superior mesenteric vein compressed by superior mesenteric artery, visualising dilatation of the jejunal vein after crossing.
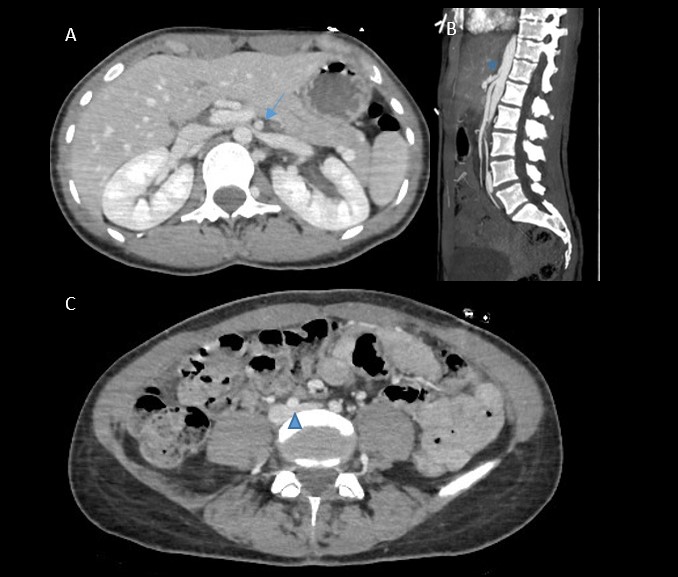
Several vascular compressions are also observed: celiac trunk stenosis of approximately 50% by arcuate ligament; severe stenosis of the left renal vein by aortomesenteric compression with compensatory drainage through hypertrophic ipsilateral lumbar veins (nutcracker syndrome); discrepancy in size between both common iliac veins, due to compression of the left iliac vein origin by the right common iliac artery, with hypertrophy of the left hypogastric vein (May-Thurner syndrome), without the patient presenting clinical symptoms secondary to these findings (Figure 2).
Figure 2
CT of the abdomen with contrast in venous phase; A. Axial section in CT of the abdomen with contrast, showing stenosis of the left renal vein due to compression between the aorta and superior mesenteric artery (nutcracker syndrome, blue arrow); B. Sagittal section, stenosis of the celiac trunk by arcuate ligament (blue star). C. Axial section, compression of the origin of the left common iliac vein by the right common iliac artery (May-Turner syndrome, blue arrowhead).
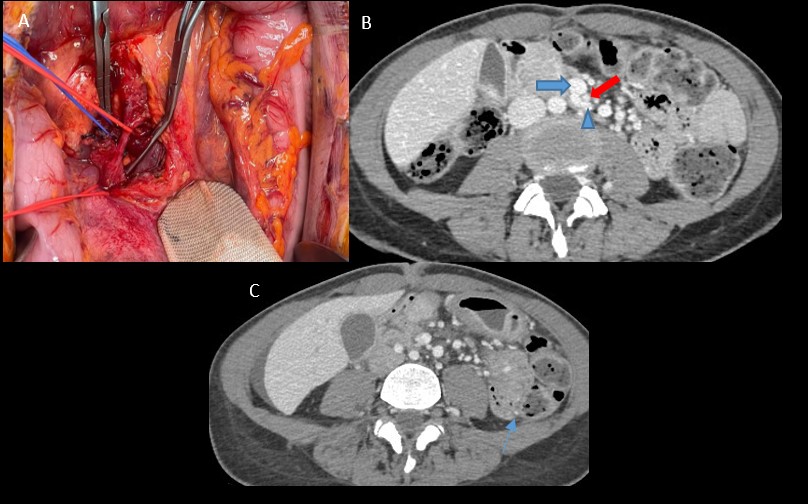
Given that the patient presented recurrent gastrointestinal bleeding with haemodynamic repercussions, it was decided to perform surgery to clamp the branch of the SMV through the SMA and the third portion of the duodenum, freeing the SMV and reducing its pressure to avoid gastrointestinal bleeding (Figure 3).
Figure 3
A. Image from the operating theatre, showing the superior mesenteric artery with red vessel loop and the superior mesenteric vein with blue. B and C. Axial slices of angio-CT of the abdomen with contrast after surgical treatment. B. Post-surgical changes with soft tissue material between SMV (marked with blue thick arrow V) and SMA (marked with red thick arrow), and decrease in calibre of the jejunal vein (blue arrowhead); C. Decrease in calibre of the jejunal submucosal varices (blue arrow) without increase in the number of varices.
The patient had a good postoperative period, with no new externalisations and stable haemoglobin levels during the 10 months of follow-up. Three months after surgery, a follow-up CT angiography of the abdomen showed post-surgical changes with a decrease in compression of the superior mesenteric vein due to an increase in the space between the SMA and SMV, as well as a significant decrease in the size of the jejunal varices.
Discussion
Compression syndromes are a rare group of pathologies[1],[2]. They most often present as incidental findings on imaging tests, although, on some occasions, they may present a characteristic clinical picture with associated morbidity. However, it is important to note that these syndromes must be accompanied by suggestive clinical features to be classified as a syndrome[3]
In our case, the patient presented with recurrent lower gastrointestinal bleeding caused by jejunal varices secondary to compression of the SMV by the SMA, which caused difficulty in venous return with a consequent increase in vascular pressure in the SMV. The SMA had an orthotopic location, with no anatomical variants. Therefore, this case serves to emphasise that not only vascular compressions with a known name[3],[4] should be recognised, but also other less frequent compressions that can cause serious pathologies and even patient mortality.
In the literature, this vascular compression is not described as a syndrome, as those reported so far correspond mostly to aortomesenteric clamp syndrome, also known as superior mesenteric artery syndrome, which consists of obstruction of the third portion of the duodenum due to compression between the SMA and the abdominal aorta, causing abdominal pain and vomiting due to difficulty in intestinal passage at this level. Normally, the third portion of the duodenum is surrounded by retroperitoneal fat, which would act as a key factor, from which it could be deduced that patients with a low BMI, as in our case, are more predisposed to suffer from these syndromes[5].
Another of the syndromes presented by the patient is May-Thurner syndrome or iliac vein compression syndrome, secondary to obstruction of the left common iliac vein caused by the crossing of the right common iliac artery[1],[2],[4],[6].
Nutcracker syndrome, also mentioned above, is uncommon and refers to the symptom complex that develops due to increased venous pressure in the left renal vein due to obstruction of its venous outflow into the inferior vena cava. Secondary to compression of the left renal vein by the aorta and SMA or, if the vein has a retroaortic course, between the aorta and the vertebral body[1],[2],[4].
Finally, arcuate ligament syndrome, or celiac artery compression syndrome, is rare and is considered to be present when narrowing of the proximal celiac trunk by the median arcuate ligament produces clinical symptoms of epigastric pain and weight loss, although these findings can also be seen in asymptomatic patients[1],[2],[4].
Imaging tests play a fundamental role not only in the evaluation of vascular structures, but also in the assessment of haemodynamic and morphological changes after vascular compression and their relationship with adjacent anatomical structures, being very useful for the surgical approach of patients requiring intervention.
Among the imaging tests, Doppler ultrasound can be used as first-line imaging, although it is highly dependent on the operator, who must have extensive experience, and is technically difficult to perform in obese individuals.
Generally, computed tomography (CT) will be the test of choice, due to its ability to produce reconstructed images, contrast resolution, multi-phase capability and non-invasiveness. The main drawback of CT is the use of ionising radiation, leaving MRI as an alternative diagnostic modality in patients allergic to iodinated contrast or when radiation exposure is a major concern, as these are usually young patients.
There are several published articles reporting cases in which a patient presents with several syndromes at the same time 7,8, one of which involved arcuate ligament syndrome and nutcracker syndrome, without seeing any relationship between the aetiology of these entities[9]. Recently, another article has been reported in which a patient presented with up to three concomitant compressive syndromes (arcuate ligament syndrome, nutcracker syndrome and aortomesenteric clamp), again with no clear relationship between these syndromes[10].There does seem to be a consensus in the literature that these types of syndromes are more frequent in young patients with little intra-abdominal fat[2],[5].
In conclusion, imaging tests play a key role in the diagnosis of infrequent causes of recurrent lower gastrointestinal bleeding in young patients in whom there may be an underlying compressive syndrome, such as ours, which has not been described in the literature.